MRI Findings Common in Neurological Disorders Key Takeaways
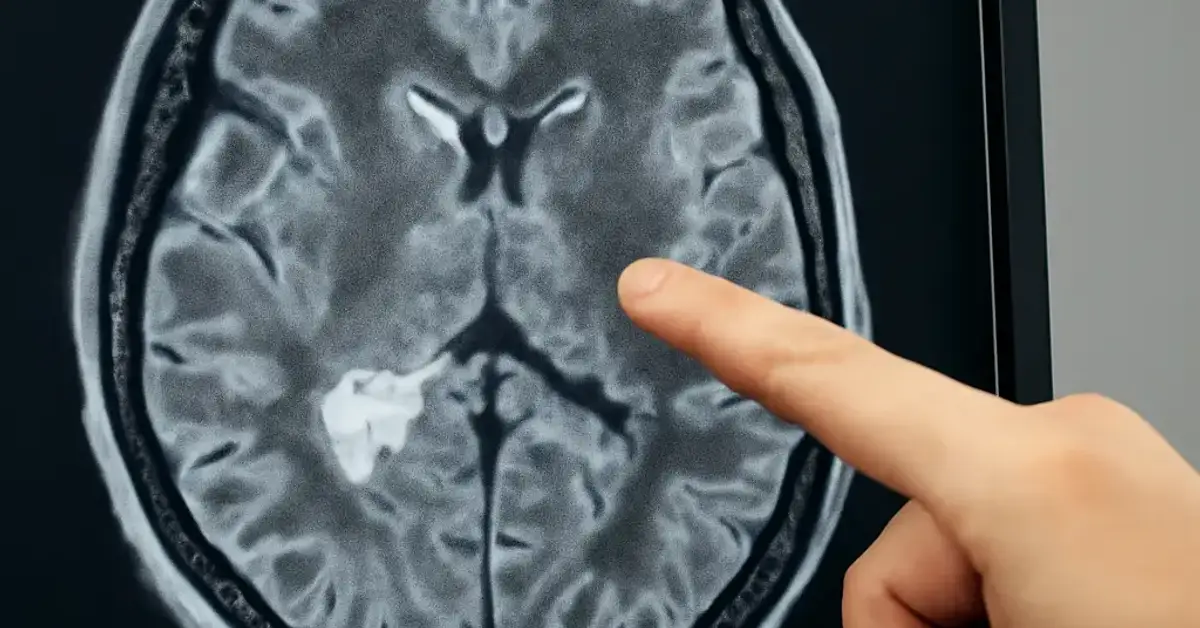
Magnetic resonance imaging (MRI) is the gold standard for visualizing structural and pathological changes in the brain and spinal cord.
- MRI Findings Common in Neurological Disorders include white matter lesions, demyelination, infarcts, tumors, hemorrhage, and brain atrophy.
- Lesion location, distribution, and enhancement patterns on MRI help distinguish between ischemic, inflammatory, infectious, and neoplastic processes.
- Contrast-enhanced MRI is critical for detecting active inflammation, blood-brain barrier breakdown, and tumor vascularity.
What Readers Should Know About MRI Findings Common in Neurological Disorders
When you open a brain MRI, the first question is often: Is this finding clinically significant? For medical students, neurology residents, and radiology trainees, being able to answer that confidently separates a novice from a competent clinician. MRI brain findings span a spectrum from normal age-related changes to life-threatening pathology. This overview focuses on nine high-yield patterns that appear frequently in clinical practice and board exams. For a related guide, see 10 Essential Neurology Investigations: A Guide for Medical Students.
Before diving into specific findings, remember that MRI exploits the magnetic properties of hydrogen protons in water and fat. T1-weighted images highlight anatomy, T2-weighted images reveal edema and inflammation, and fluid-attenuated inversion recovery (FLAIR) suppresses cerebrospinal fluid to make periventricular lesions more conspicuous. Diffusion-weighted imaging (DWI) captures acute ischemia, while gradient-echo (GRE) sequences detect hemorrhage. Each sequence contributes to a complete neurological MRI interpretation.
1. White Matter Lesions on MRI: Common Yet Clinically Critical
White matter lesions MRI are hyperintense foci on T2 and FLAIR sequences. They reflect demyelination, axonal loss, or small-vessel ischemia. In older adults, periventricular and deep white matter hyperintensities often indicate chronic microvascular disease from hypertension or diabetes. In younger patients, especially women, white matter lesions raise suspicion for multiple sclerosis MRI findings when they are ovoid, perivenular, and located in the corpus callosum, periventricular regions, or juxtacortical areas.
What do white matter lesions on MRI mean?
Not all white matter lesions are pathological. Mild punctate lesions can be incidental, especially in migraineurs or individuals with cardiovascular risk factors. However, confluent, progressive, or enhancing lesions warrant further workup. The Fazekas scale grades severity: grade 0 (no lesions), grade 1 (punctate foci), grade 2 (beginning confluence), and grade 3 (large confluent areas). This grading helps communicate the burden of demyelinating disease MRI changes.
2. Demyelinating Lesions: Hallmarks of Multiple Sclerosis
Demyelinating disease MRI features are defined by lesion distribution, morphology, and enhancement. In multiple sclerosis (MS), classic findings include Dawson’s fingers — ovoid lesions perpendicular to the lateral ventricles along medullary veins. Active plaques enhance with contrast, indicating blood-brain barrier disruption. Chronic lesions appear as black holes on T1-weighted images, signifying irreversible axonal loss.
What MRI findings suggest multiple sclerosis?
The McDonald criteria incorporate MRI findings to diagnose MS. Look for at least one T2-hyperintense lesion in at least two of four CNS areas: periventricular, cortical/juxtacortical, infratentorial, and spinal cord. Dissemination in space and time — new T2 lesions or gadolinium-enhancing lesions on follow-up MRI — confirms active disease. Multiple sclerosis MRI remains the most sensitive imaging modality for diagnosing and monitoring MS.
3. Acute Infarcts on Diffusion-Weighted Imaging
Stroke MRI imaging is incomplete without DWI. Acute ischemic strokes appear as bright areas on DWI with corresponding low signal on apparent diffusion coefficient (ADC) maps within minutes of symptom onset. This is the most sensitive and specific finding for acute infarction. Large-vessel occlusions cause territorial infarcts, while lacunar infarcts involve small penetrating arteries supplying the basal ganglia, thalamus, and internal capsule.
How is stroke seen on MRI scans?
On T2 and FLAIR, acute infarcts become hyperintense after 6–12 hours. Hemorrhagic transformation shows blooming on GRE sequences. MRI also differentiates acute from chronic infarcts: acute lesions restrict diffusion, whereas chronic infarcts are encephalomalacic with FLAIR suppression. This distinction is vital for guiding thrombolysis decisions and assessing prognosis.
4. Brain Tumors: Recognizing Mass Effect and Enhancement Patterns
Brain tumor MRI interpretation relies on location, signal characteristics, enhancement, and surrounding vasogenic edema. Glioblastomas typically cause irregular ring enhancement with central necrosis on T1 post-contrast. Meningiomas are extra-axial, dural-based, and enhance homogeneously, often with a dural tail. Metastases are multiple, round, and located at the gray-white matter junction with intense ring enhancement and marked edema.
How do brain tumors appear on MRI?
Low-grade gliomas like astrocytomas appear as T2 hyperintense, T1 hypointense masses without enhancement. High-grade tumors show heterogeneous enhancement due to neovascularity and blood-brain barrier breakdown. Contrast MRI brain studies are essential for assessing tumor grade, surgical planning, and monitoring treatment response. For a related guide, see Neurological Conditions: Symptoms, Signs, and Treatment.
5. Hemorrhage: The Unique Role of Susceptibility-Weighted Imaging
MRI brain findings of hemorrhage depend on the age of the blood product. Acute hemorrhage (< 24 hours) is isointense on T1 and hypointense on T2 due to deoxyhemoglobin. Subacute hemorrhage (days to weeks) becomes hyperintense on T1 due to methemoglobin, and chronic hemorrhage (weeks to months) leaves a hypointense rim of hemosiderin on GRE/SWI. These sequences are incredibly sensitive for detecting microbleeds in cerebral amyloid angiopathy and hypertensive small-vessel disease.
6. Brain Atrophy: Patterns That Indicate Neurodegeneration
Brain atrophy MRI is more than global volume loss; regional patterns point to specific neurodegenerative diseases. Alzheimer disease shows disproportionate medial temporal lobe and hippocampal atrophy. Frontotemporal dementia affects the frontal and anterior temporal lobes with relative sparing of posterior regions. Lewy body dementia often combines mild diffuse atrophy with occipital hypoperfusion.
What does brain atrophy indicate on MRI?
While mild atrophy is a normal aging process, accelerated or focal atrophy suggests a pathological process. Neurodegenerative MRI findings include cortical thinning, ventricular enlargement, and loss of gray-white matter differentiation. Serial MRIs can track disease progression and guide treatment decisions in conditions like Alzheimer disease, Parkinson disease, and multiple system atrophy.
7. Infections: Leptomeningeal and Parenchymal Patterns
Neurological imaging patterns of CNS infections include leptomeningeal enhancement (bacterial meningitis), ring-enhancing lesions (brain abscesses), and periventricular T2 hyperintensity (herpes simplex encephalitis). Tuberculomas appear as small ring-enhancing nodules with central caseation. Neurocysticercosis shows cyst-like lesions with a scolex (visible dot inside the cyst). MRI with contrast is indispensable for detecting active inflammation and associated complications such as ventriculitis or cerebritis.
How are infections shown on MRI brain imaging?
FLAIR hyperintensity in the subarachnoid spaces and leptomeningeal enhancement on post-contrast T1 are classic for meningitis. Abscesses show a smooth, thin rim of enhancement with central restricted diffusion. Contrast MRI brain helps differentiate infection from tumor and guides lumbar puncture timing.
8. Epilepsy-Related MRI Changes
MRI brain findings in epilepsy patients often reveal structural abnormalities such as hippocampal sclerosis, cortical dysplasias, tumors, and vascular malformations. Hippocampal sclerosis is the most common cause of temporal lobe epilepsy and appears as T2/FLAIR hyperintensity and volume loss in the hippocampus, best seen on coronal oblique sequences. Focal cortical dysplasias show transmantle signal changes and blurring of the gray-white matter junction.
What MRI changes are seen in epilepsy patients?
Up to 30% of patients with refractory epilepsy have a detectable lesion on dedicated epilepsy protocol MRI (thin-slice T2, FLAIR, and 3D T1 sequences). Identifying these lesions is crucial for surgical planning and achieving seizure freedom. Clinical neuroradiology emphasizes the importance of high-resolution imaging for this population.
9. Contrast Enhancement Patterns: The Key to Differentiating Active Disease
Contrast MRI brain is not always necessary, but when used, enhancement patterns provide diagnostic clarity. Nodular or ring enhancement suggests active demyelination, tumor, or abscess. Leptomeningeal enhancement points to infection, sarcoidosis, or carcinomatous meningitis. Pial enhancement can be seen in meningitis or stroke. Radiology neurology MRI protocols often include contrast to answer specific clinical questions: Is this an active MS plaque? Is this a high-grade glioma? Is there blood-brain barrier breakdown?
How does contrast enhancement help MRI diagnosis?
Gadolinium-based contrast agents shorten T1 relaxation time, making enhancing structures bright on T1-weighted images. Enhancement indicates inflammation, neovascularity, or disruption of the normal blood-brain barrier. In MS, enhancement confirms active inflammation. In tumors, enhancement pattern guides grading and biopsy targeting.
How MRI Differentiates Acute vs. Chronic Lesions in Neurological Disorders
Differentiating acute from chronic lesions is a daily task in neuroimaging diagnosis. Acute infarcts show DWI positivity for up to 10–14 days. Chronic infarcts appear as T2/FLAIR hyperintense cavities with surrounding gliosis and no DWI signal. Acute MS plaques enhance; chronic plaques do not. Acute hemorrhage evolves through predictable stages on T1 and T2 images, while chronic hemorrhage leaves hemosiderin staining on GRE. Recognizing these temporal patterns is essential for accurate staging and management.
How does MRI differentiate acute and chronic lesions?
The combination of DWI, contrast-enhanced T1, and susceptibility-weighted sequences allows radiologists to date lesions. Acute lesions restrict diffusion, enhance, or show acute blood products. Chronic lesions show T2/FLAIR hyperintensity without DWI positivity, no enhancement, and hemosiderin deposition. Neurological imaging patterns are time-sensitive, and this knowledge directly impacts treatment decisions such as thrombolysis, steroids, or antibiotics.
Why MRI Is the Gold Standard in Clinical Neuroradiology
Clinical neuroradiology relies on MRI for its superior soft-tissue contrast, multiplanar capability, and ability to characterize tissue composition without ionizing radiation. Unlike CT, MRI can distinguish between gray and white matter, visualize the posterior fossa without artifact, and detect subtle lesions like cortical dysplasia or small-vessel ischemia. Neurological MRI protocols can be tailored to answer specific clinical questions — stroke, tumor, infection, epilepsy, or neurodegeneration — making it indispensable in modern neurology.
High-Yield MRI Findings for Exams: What Trainees Must Know
For exam preparation, remember the following high-yield associations:
- Multiple sclerosis: Ovoid T2 hyperintensities in periventricular, juxtacortical, infratentorial, and spinal cord regions; contrast-enhancing active plaques; Dawson’s fingers.
- Acute ischemic stroke: DWI positive with ADC correlate; large territorial or lacunar pattern.
- Glioblastoma: Irregular ring enhancement with central necrosis, thick walls, and surrounding edema.
- Meningioma: Extra-axial, dural-based, homogeneous enhancement with dural tail.
- Brain atrophy in Alzheimer disease: Medial temporal and hippocampal volume loss out of proportion to age.
- CNS infection: Leptomeningeal enhancement or ring-enhancing abscesses with restricted diffusion.
- Hippocampal sclerosis: T2/FLAIR hyperintensity and volume loss in the hippocampus, the most common surgical target in epilepsy.
Mastering these high yield MRI findings for exams will serve you throughout your clinical career and board examinations.
Useful Resources
For deeper understanding of MRI Findings Common in Neurological Disorders, explore these authoritative resources:
- Radiopaedia: Brain MRI — Comprehensive review of protocols, sequences, and pathological findings
- NIH: Neuroimaging in Neurological Disorders — A thorough primer on MRI, CT, and PET applications
Frequently Asked Questions About MRI Findings Common in Neurological Disorders
What are common MRI findings in neurological disorders?
Common findings include white matter hyperintensities, acute and chronic infarcts, demyelinating plaques (e.g., multiple sclerosis), brain tumors (e.g., glioblastoma, meningioma), hemorrhage, brain atrophy (especially in neurodegenerative diseases), and leptomeningeal enhancement from infection or inflammation.
How does MRI detect brain abnormalities?
MRI uses strong magnetic fields and radiofrequency pulses to generate images based on water and fat content. T1-weighted images show anatomy; T2 and FLAIR highlight edema and inflammation; DWI detects acute ischemia; GRE/SWI reveals hemorrhage; and contrast-enhanced T1 shows blood-brain barrier breakdown. Together, these sequences help identify structural and pathological changes.
What do white matter lesions on MRI mean?
White matter lesions are T2/FLAIR hyperintensities that can represent small-vessel ischemic disease (common with aging and hypertension), demyelination (as in MS), or inflammatory changes. Their location, morphology, and enhancement pattern help determine clinical significance.
How is stroke seen on MRI scans?
Acute ischemic stroke appears as a bright area on DWI with corresponding low ADC signal. On T2/FLAIR, it becomes hyperintense after 6–12 hours. Chronic infarcts are T2/FLAIR hyperintense cavities without DWI positivity and often with surrounding gliosis. Hemorrhagic strokes show blooming on GRE.
What MRI findings suggest multiple sclerosis?
Classic MS findings include ovoid T2 hyperintensities in periventricular, juxtacortical, infratentorial, and spinal cord regions, often perpendicular to the ventricles (Dawson’s fingers). Active plaques enhance with contrast. The McDonald criteria require dissemination in space and time.
How do brain tumors appear on MRI?
Brain tumors vary by type. Glioblastomas show irregular ring enhancement with necrosis and edema. Meningiomas are extra-axial, dural-based, and enhance homogeneously. Metastases are multiple, round, at the gray-white junction, with ring enhancement and extensive vasogenic edema. Low-grade gliomas appear as T2 hyperintense, non-enhancing masses.
What does brain atrophy indicate on MRI?
Brain atrophy can be a normal age-related finding or indicate neurodegenerative disease. Alzheimer disease typically shows disproportionate medial temporal and hippocampal atrophy. Frontotemporal dementia affects the frontal and temporal lobes. Serial MRI helps differentiate pathological from physiological atrophy.
How are infections shown on MRI brain imaging?
CNS infections present with leptomeningeal enhancement (meningitis), ring-enhancing lesions with restricted diffusion (abscesses), or T2 hyperintensity in the temporal lobes (herpes encephalitis). Contrast-enhanced MRI is critical for detecting active inflammation and complications.
What MRI changes are seen in epilepsy patients?
Common findings include hippocampal sclerosis (T2/FLAIR hyperintensity and volume loss), focal cortical dysplasias (blurring of gray-white junction and transmantle signal), tumors, and vascular malformations. Dedicated epilepsy protocol MRI increases detection rates.
How does MRI differentiate acute and chronic lesions?
Acute lesions (infarcts, active MS plaques) are DWI-positive and may enhance with contrast. Chronic lesions show T2/FLAIR hyperintensity without DWI positivity, no enhancement, and may show gliosis or atrophy. Hemorrhage evolves through predictable T1/T2 stages; chronic stages show hemosiderin on GRE.
What are demyelinating lesions on MRI?
Demyelinating lesions are T2/FLAIR hyperintensities caused by loss of myelin. They are characteristic of multiple sclerosis and other demyelinating diseases. Key features include ovoid shape, perivenular distribution, and presence in typical locations (periventricular, juxtacortical, infratentorial, spinal cord).
How do radiologists interpret neurological MRI scans?
Radiologists follow a systematic approach: assess patient history, review all sequences (T1, T2, FLAIR, DWI, GRE, post-contrast), identify lesions by signal and location, and correlate with clinical context. They use standardized reporting and scoring systems (e.g., Fazekas, McDonald criteria) for consistency.
What are high yield MRI findings for exams?
High-yield findings include DWI-positive infarcts, ovoid periventricular lesions in MS, ring-enhancing glioblastoma, extra-axial dural-based meningioma, hippocampal sclerosis in epilepsy, and confluent white matter changes in microvascular disease. Knowing these patterns helps answer board-style questions quickly.
How does contrast enhancement help MRI diagnosis?
Contrast agents accumulate in areas of blood-brain barrier breakdown, active inflammation, and tumor neovascularity. Enhancement identifies active MS plaques, differentiates high-grade from low-grade tumors, detects meningitis and abscesses, and helps characterize vascular malformations and infarction.
What MRI patterns suggest neurodegenerative disease?
Alzheimer disease: disproportionate hippocampal and medial temporal atrophy. Frontotemporal dementia: frontal and anterior temporal atrophy with relative posterior sparing. Lewy body dementia: mild diffuse atrophy with occipital hypoperfusion. Progressive supranuclear palsy: midbrain atrophy (hummingbird sign). Multiple system atrophy: pontine and cerebellar atrophy (hot cross bun sign).
How does MRI visualize spinal cord pathology?
Spinal cord MRI uses T1, T2, STIR, and post-contrast sequences. Common findings include demyelinating plaques (MS), compressive myelopathy from disc herniation or stenosis, intramedullary tumors (ependymoma, astrocytoma), vascular malformations, and inflammatory lesions in transverse myelitis.
What is the role of FLAIR sequence in neurological MRI ?
FLAIR (fluid-attenuated inversion recovery) suppresses the signal from CSF, making periventricular and cortical lesions more visible. It is particularly useful for detecting MS plaques, subarachnoid hemorrhage, meningitis, and edema adjacent to the ventricles.
When is contrast-enhanced MRI necessary in neurological imaging?
Contrast is indicated when evaluating suspected tumor, active infection, demyelinating disease (to assess activity), meningitis, and leptomeningeal disease. It is not routinely needed for acute stroke unless ruling out tumor mimics or evaluating for hemorrhagic transformation.
How do you differentiate between ischemic and hemorrhagic stroke on MRI?
Ischemic stroke appears as DWI-positive restricted diffusion with T2/FLAIR hyperintensity after a few hours. Hemorrhagic stroke shows blooming on GRE/SWI and evolves through predictable T1/T2 stages: acute (< 24 h) is T2 hypointense, subacute (days) is T1 hyperintense, chronic shows hemosiderin rim.
What is the differential for ring-enhancing brain lesions on MRI?
Differential includes glioblastoma (irregular, thick walls, central necrosis), brain abscess (smooth, thin rim, restricted diffusion), metastasis (multiple, at gray-white junction, surrounding edema), tumefactive demyelination (open-ring pattern), and toxoplasmosis (basal ganglia, ring with eccentric nodule in immunocompromised).
