Using an inhaler correctly is one of the most important factors in effective asthma control, and global strategies such as the Global Initiative for Asthma (GINA) 2025 strategy report highlight poor technique as a major cause of preventable flare‑ups and uncontrolled symptoms. Proper technique ensures that medication reaches the lower airways instead of staying in the mouth or throat, which leads to better symptom control, fewer attacks, and reduced emergency visits as echoed in practical inhaler guides from the American Lung Association.
Why Proper Inhaler Technique Matters
Incorrect inhaler use can result in:
- Medication staying in the mouth or throat
- Poor delivery to the lower airways
- Ongoing wheezing and breathlessness
- Increased risk of asthma attacks
Many people believe their medication “isn’t working” when the real issue is inhaler technique, a problem frequently noted in asthma audits summarized by GINA. Proper inhaler technique helps:
- Ensure maximum medication reaches the lungs
- Provide faster symptom relief
- Improve long-term inflammation control
- Reduce urgent care and ER visits
If you want to see how inhaler technique fits into the bigger picture of triggers, medications, and monitoring, you can frame this guide alongside your main article on asthma management: triggers, treatment, and prevention.
Understanding Your Asthma Before Using an Inhaler
Before focusing on technique, it helps to understand:
- What typically triggers your asthma
- When to use your quick‑relief (rescue) inhaler
- When and how to use your daily controller inhaler
If you are unsure what worsens your symptoms, review your dedicated resource on common asthma triggers, which covers allergens, infections, smoke, pollution, and other everyday exposures.
Every person with asthma should also have a structured written plan describing when to adjust medicines and when to seek help; if you do not yet have one, you can follow your step‑by‑step framework in the article on creating an asthma action plan.
Types of Inhalers | How to Use Inhaler Correctly
Different inhalers require different techniques, which is why guidelines distinguish device‑specific instructions in their inhaler education materials.
Common types include:
- Metered‑Dose Inhaler (MDI)
- Dry Powder Inhaler (DPI)
- Soft Mist Inhaler
- Nebulizer
This guide focuses on MDIs and DPIs, which are the most frequently prescribed home devices and are also highlighted in patient‑facing inhaler instructions from the American Lung Association.
How to Use a Metered‑Dose Inhaler (MDI)
A metered‑dose inhaler delivers medication in aerosol form and works best with slow, steady inhalation coordinated with the spray.
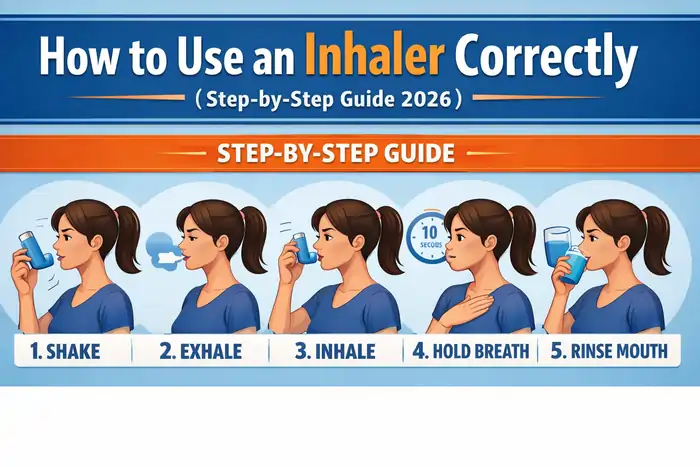
Step‑by‑Step Instructions
- Remove the cap and shake the inhaler well for 5–10 seconds.
- Sit or stand upright so your lungs can expand fully.
- Exhale fully away from the inhaler to empty your lungs.
- Place the mouthpiece between your lips and seal tightly.
- Begin inhaling slowly through your mouth.
- As you start to breathe in, press down on the inhaler once.
- Continue inhaling slowly and deeply for about 3–5 seconds.
- Hold your breath for up to 10 seconds if you can.
- Exhale gently through your mouth or nose.
If more than one puff is prescribed, wait about 30–60 seconds between puffs and repeat the steps. Many step‑by‑step diagrams from groups like the American Lung Association mirror this sequence closely.
Common Mistakes With MDIs
Frequent technique errors include:
- Inhaling too quickly
- Spraying before or after you start inhaling
- Not shaking the inhaler
- Forgetting to hold your breath
- Not using a spacer when recommended
Even minor mistakes can significantly reduce medication delivery to the lungs, which is why GINA recommends reviewing technique regularly in its asthma strategy documents.
Should You Use a Spacer?
A spacer (or valved holding chamber) attaches to an MDI and makes it easier to get the medicine into your lungs.
Benefits:
- Improves drug delivery
- Reduces throat irritation
- Makes timing less critical
Especially helpful for:
- Children
- Older adults
- Anyone with coordination difficulties
Using a spacer correctly:
- Shake the inhaler and insert it into the spacer.
- Place the spacer mouthpiece in your mouth (or mask over nose and mouth) and seal.
- Press the inhaler once to release a puff into the chamber.
- Inhale slowly and deeply through the spacer.
- Hold your breath for about 10 seconds before exhaling.
Many asthma management plans, including those aligned with GINA recommendations, explicitly encourage spacer use with MDIs, especially for children. For a broader look at how spacers fit into daily control, you can link back to your main asthma management guide when you mention “daily asthma control strategies.”
How to Use a Dry Powder Inhaler (DPI)
Dry powder inhalers deliver medication as a fine powder and rely on your own strong, deep breath to pull the medicine into the lungs.
Step‑by‑Step Instructions
- Prepare or load the dose according to the device’s instructions (twist, slide, click, or open as directed).
- Exhale fully away from the inhaler (never into the mouthpiece).
- Place the mouthpiece in your mouth and form a tight seal.
- Inhale quickly and deeply through your mouth.
- Hold your breath for about 10 seconds if possible.
- Exhale slowly, away from the device.
Important reminders:
- Do not shake a DPI unless the instructions specifically tell you to.
- Do not blow into the device, as moisture can clump the powder and block the dose.
Device‑specific patient leaflets often illustrate these steps, and they match the general DPI approach used in many educational videos and handouts.
After Using an Inhaled Corticosteroid
If your inhaler contains an inhaled corticosteroid (ICS) such as fluticasone or budesonide:
- Rinse your mouth with water after each use.
- Gargle and spit the water out (do not swallow).
This simple step reduces the risk of oral thrush and hoarseness, side effects that are discussed in ICS safety summaries and patient information from major respiratory organizations. ICS remain the first‑line maintenance therapy for persistent asthma in global guidelines like the GINA 2025 report.
How Often Should Inhaler Technique Be Reviewed?
Clinical guidelines recommend reviewing inhaler technique:
- At every asthma follow‑up visit
- After any change in device or medication
- Whenever asthma control worsens or rescue inhaler use increases
Experts regularly point out that even experienced patients drift into bad habits, which is why technique checks are included in routine asthma reviews.
Signs Your Inhaler Technique May Be Incorrect
Consider having your technique reassessed if you notice:
- Frequent wheezing or chest tightness
- Nighttime coughing or waking due to symptoms
- Needing your rescue inhaler more often than usual
- Lower than usual peak flow readings
- Poor or short‑lived relief after using your inhaler
In practice, clinicians often review inhaler technique before stepping up therapy, since incorrect use is such a common cause of “uncontrolled” asthma.
Inhaler Use in Children
Children often require:
- A spacer with a mask rather than a mouthpiece
- Close caregiver supervision
- Demonstration plus “teach‑back” where they show the technique back
Teaching proper inhaler use early helps prevent long‑term complications and aligns with pediatric asthma education approaches used in school‑based programs and pediatric clinics. Parents and caregivers should also understand environmental triggers; you already cover this in detail in your article on common asthma triggers.
Inhaler Use in Older Adults
Older adults may face challenges such as:
- Reduced hand strength
- Arthritis or limited dexterity
- Poor coordination or cognitive decline
In these situations, switching to easier devices (such as MDIs with spacers, soft‑mist inhalers, or nebulizers) and simplifying steps can improve medication delivery. Many geriatric asthma reviews emphasize tailoring the device choice to a person’s abilities rather than using a one‑size‑fits‑all approach.
Integrating Inhaler Use Into Your Asthma Action Plan
Your inhaler schedule should follow your written asthma action plan:
- Green zone: daily controller inhaler use when you feel well.
- Yellow zone: which inhaler to use and how often when symptoms start to worsen.
- Red zone: when to use multiple reliever doses and when to seek emergency care.
For readers who don’t yet have a plan, you can embed a natural internal link when you mention “written asthma action plan” or “emergency steps,” pointing them to your guide on building an asthma action plan.
Frequently Asked Questions
How do I know if my inhaler is empty?
Many newer inhalers have a built‑in dose counter; if yours does not, your pharmacist or clinician can help you calculate how many doses are in each device and set a replacement schedule.
Can I share my inhaler?
No. Inhalers are prescribed medications tailored to an individual’s condition and dose and should never be shared.
Why is holding my breath important?
Holding your breath briefly after inhalation allows medicine particles to settle deeper into your lungs instead of being exhaled immediately.
Is shaking always required?
Shake MDIs before each use unless the instructions say otherwise; DPIs generally should not be shaken.
When to Seek Medical Attention
Seek urgent or emergency care if:
- Your rescue inhaler does not relieve symptoms
- You cannot speak full sentences because of shortness of breath
- Your lips or fingernails turn blue or gray
- Your breathing becomes severely labored or you see chest retractions
For a broader look at emergency steps and long‑term prevention, it’s helpful to guide readers back to your main asthma management article when discussing severe symptoms and escalation.
⚠️ Medical Disclaimer
The information provided on MedEduHub is for educational purposes only and does not replace professional medical advice, diagnosis, or treatment.
If you experience severe breathing difficulty, inability to speak, chest retractions, or signs of respiratory distress, seek emergency medical care immediately.
Always consult a licensed healthcare provider before starting, stopping, or changing any asthma treatment plan.
Written by: Eden Grace Ramos-Arsenio, RN
📚 Medical Sources & References
- This article is based on current clinical guidelines and peer-reviewed research from:
- Peer-reviewed respiratory medicine journals
- Global Initiative for Asthma (GINA) 2025 Strategy Report
- World Health Organization (WHO) Asthma Fact Sheet
- Centers for Disease Control and Prevention (CDC) Asthma Control Resources
- American Lung Association Inhaler Technique Guidance
