Hypothyroidism, or underactive thyroid, happens when your thyroid gland does not make enough thyroid hormone to meet your body’s needs. When hormone levels are low, many of your body’s functions slow down, which can affect your energy, weight, mood, heart, and digestion.
This guide gives a clear, patient‑friendly overview; you can also explore our main page at Hypothyroidism (Underactive Thyroid) and trusted resources from NIDDK/NIH, Cleveland Clinic, and the American Thyroid Association.
What Is Hypothyroidism?
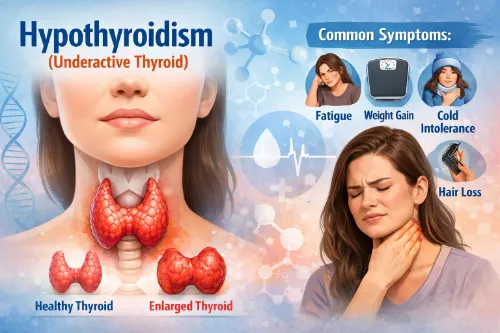
Hypothyroidism is a condition in which the thyroid gland, a small butterfly-shaped gland located at the base of your neck, does not produce enough thyroid hormones—primarily thyroxine (T4) and triiodothyronine (T3). These hormones play a crucial role in regulating your body’s metabolism, or how your body converts food into energy.
When hormone levels are too low, your body processes start to slow down, affecting vital organs such as your heart, brain, muscles, and digestive system.
Because the thyroid helps control metabolism, low thyroid activity can influence nearly every system in the body. Without enough thyroid hormones, many people experience fatigue, sluggishness, weight gain, dry skin, constipation, and a sensitivity to cold temperatures.
Mental health can also be affected—some individuals report memory problems, difficulty concentrating, or low mood. These symptoms often develop gradually over several months or years and may initially be mistaken for aging, stress, or other health concerns.
Common Symptoms of Hypothyroidism
Symptoms can vary from person to person and may be mild at first. Many people notice symptoms only gradually over months or years.
Typical symptoms include:
- Fatigue and low energy – feeling unusually tired, even after a full night’s sleep.
- Weight gain or difficulty losing weight – often modest but frustrating, even without big changes in diet.
- Feeling cold easily – trouble tolerating cold temperatures when others are comfortable.
- Dry skin and dry, thinning hair – skin may feel rough; hair can become coarse or fall out more than usual.
- Constipation and bloating – slowed digestion is common.
- Low mood or depression – feeling down, less motivated, or “foggy.”
- Slow heart rate – sometimes noticed as feeling sluggish or easily winded.
- Muscle and joint aches – stiffness, cramps, or general body aches.
Symptoms in Women
Women are more likely to develop hypothyroidism, especially from autoimmune causes like Hashimoto’s disease. Additional features can include:
- Heavy, irregular, or less frequent periods.
- Fertility problems or difficulty getting pregnant.
- Symptoms that worsen during or after pregnancy (postpartum thyroiditis).
Symptoms in Men
Men can also develop hypothyroidism, but it may be missed if symptoms are attributed to stress or aging.
They may notice:
- Reduced sex drive (low libido) or erectile problems.
- Tiredness, reduced exercise tolerance, and muscle weakness.
- Mood changes, such as low mood, irritability, or poor concentration.
Because these symptoms can overlap with many other conditions, blood tests are essential to confirm the diagnosis.
What Happens in the Body?
When the thyroid is underactive, it does not release enough T4 and T3 into the bloodstream. The pituitary gland senses this and produces more thyroid‑stimulating hormone (TSH) to try to “push” the thyroid to work harder. As a result:
- TSH is often high.
- Free T4 (and sometimes T3) is low or at the low end of normal.
This hormonal pattern slows processes such as heart rate, heat production, and how quickly cells use oxygen and calories. In some people, TSH is raised but T4 is still in the normal range (subclinical hypothyroidism), which may or may not cause symptoms.
Most Common Causes of Hypothyroidism
Hypothyroidism can arise from problems in the thyroid itself (primary hypothyroidism) or, much less often, from issues with the pituitary or hypothalamus (secondary or central hypothyroidism).
Major causes include:
1. Hashimoto’s Disease (Autoimmune Thyroiditis)
Hashimoto’s disease is the most common cause of hypothyroidism in many countries. It is an autoimmune disorder in which the immune system attacks the thyroid, causing long‑term inflammation and gradual loss of function. Over time, the gland can no longer make enough hormone, leading to permanent hypothyroidism that usually needs lifelong treatment.
2. Thyroid Surgery and Radioactive Iodine
- Thyroid surgery (thyroidectomy) – removal of part or all of the thyroid for nodules, goiter, or cancer often results in an underactive thyroid.
- Radioactive iodine therapy – used to treat hyperthyroidism or toxic nodules; the treatment can destroy much of the thyroid tissue, causing hypothyroidism later.
In these cases, hypothyroidism is expected and managed with thyroid hormone replacement.
3. Thyroiditis (Inflammation)
Different forms of thyroiditis (such as painless, subacute, or postpartum thyroiditis) can initially cause a “leak” of stored hormone and temporary hyperthyroidism, followed by hypothyroidism once stores are depleted. In some people, the underactive phase is temporary; in others, it becomes permanent.
4. Iodine Imbalance
Iodine is essential for thyroid hormone production.
- Too little iodine (still an issue in some regions) can cause goiter and hypothyroidism.
- Too much iodine from supplements or certain medications can also interfere with hormone production and trigger hypothyroidism in susceptible people.
5. Medications and Other Conditions
Some medicines and health problems can affect thyroid function.
Examples include:
- Amiodarone, lithium, some cancer and immune‑modulating therapies.
- Previous radiation to the neck or head.
- Other autoimmune conditions (type 1 diabetes, celiac disease, rheumatoid arthritis, lupus, pernicious anaemia) which increase the risk of autoimmune thyroid disease.
How Hypothyroidism Is Diagnosed
Diagnosis is based on symptoms plus blood tests, and sometimes imaging.
Key tests:
- TSH (thyroid‑stimulating hormone) – usually high in primary hypothyroidism.
- Free T4 (thyroxine) – often low or low‑normal.
- Thyroid antibodies (TPOAb, sometimes TgAb) – can help confirm autoimmune causes like Hashimoto’s disease.
- In overt hypothyroidism, TSH is high and free T4 is low.
- In subclinical hypothyroidism, TSH is raised but free T4 is still in the normal range.
Ultrasound may be used if there is a goiter or nodules, but many people with hypothyroidism do not need imaging.
Treatment and Long‑Term Management
The main treatment for hypothyroidism is thyroid hormone replacement. Treatment aims to restore hormone levels to a healthy range and relieve symptoms, not to “boost” thyroid beyond normal.
Levothyroxine
Levothyroxine is a synthetic form of T4 that works the same way as your natural hormone.
- Usually taken once daily, on an empty stomach with water.
- Most people take it in the morning and wait 30–60 minutes before eating or drinking anything besides water.
- The dose is adjusted over time based on TSH (and sometimes free T4) and how you feel.
In most cases, treatment is lifelong, but doses may change with age, weight changes, pregnancy, or other illnesses.
Subclinical Hypothyroidism
If TSH is only slightly raised and T4 is normal, your provider may recommend “watchful waiting” with repeat tests rather than immediate treatment. Treatment is more likely to be suggested if:
- TSH is significantly elevated.
- You have symptoms, positive thyroid antibodies, heart disease, or are pregnant or trying to conceive.
Possible Complications if Left Untreated
When properly treated, hypothyroidism is usually well controlled and complications are uncommon. If it is not treated or the dose is very inadequate, risks can include:
- High cholesterol and increased risk of heart disease.
- High blood pressure and heart failure in severe or long‑standing cases.
- Infertility and pregnancy complications.
- Nerve problems such as carpal tunnel syndrome.
- Very rarely, a life‑threatening state called myxoedema coma, usually in older people with severe, long‑term untreated hypothyroidism.
Regular follow‑up and the right dose of medicine help prevent these problems for most people.
Living Well with Hypothyroidism
Most people with hypothyroidism can live normal, active lives once they are on the right dose of medication. Good day‑to‑day management focuses on:
- Taking levothyroxine correctly and consistently.
- Keeping regular blood test appointments (usually every 6–12 months when stable, or more often while adjusting).
- Talking to your healthcare provider if symptoms persist or return, as your dose may need adjustment.
- Discussing pregnancy plans early, as doses often need to be increased in pregnancy.
You can find additional practical tips in patient pages from NIDDK, Healthdirect, and the ATA.
Pro Tip for Daily Living with Hypothyroidism
- Take levothyroxine at the same time every day, on an empty stomach with water, and wait at least 30–60 minutes before breakfast or coffee to improve absorption.
- Avoid taking calcium, iron, or multivitamins within 4 hours of your thyroid pill, as they can reduce how much medicine your body absorbs.
- If you miss a dose, most guidelines allow you to take it when you remember later that day, or take two tablets the next day if your doctor has advised this—never change your routine without checking first.
- Keep a simple log (or phone note) of symptoms, blood test dates, and dose changes and bring it to appointments; this helps your provider fine‑tune your dose more easily.
- Tell your doctor or pharmacist you take levothyroxine whenever a new long‑term medication is prescribed, as some drugs can interact and affect your thyroid levels.
Frequently Asked Questions
1. Can hypothyroidism be cured, or is it always permanent?
In many people, hypothyroidism is long‑term and requires lifelong treatment, especially when caused by Hashimoto’s disease, surgery, or radioactive iodine. In some cases linked to temporary thyroiditis, hormone levels can return to normal over time and medicine may be reduced or stopped under medical guidance.
2. How long does it take to feel better after starting levothyroxine?
Most people notice some improvement in symptoms within a few weeks, but it can take several months to feel the full benefits as hormone levels and dosage are fine‑tuned. Follow‑up blood tests are usually done every 6–8 weeks at first to adjust the dose until TSH and T4 are in the target range.
3. Do I need to follow a special diet for hypothyroidism?
There is no single “hypothyroid diet,” but a balanced diet with enough iodine, selenium, and iron supports overall thyroid health. Excessive intake of iodine, very high‑dose supplements, or extreme restrictive diets can sometimes worsen thyroid balance and should be discussed with your healthcare provider.
4. Are there foods or drinks I should avoid with my thyroid medication?
Some foods and drinks—such as high‑fiber meals, soy products, coffee, and grapefruit juice—can reduce how well levothyroxine is absorbed if taken too close to your dose. Taking your tablet on an empty stomach with water and waiting before food or coffee helps your body absorb the full dose.
5. Can I take my levothyroxine at night instead of in the morning?
Yes, some people successfully take levothyroxine at bedtime, as long as it is taken on an empty stomach at least 3–4 hours after the last meal. The most important thing is to choose a time you can consistently take it the same way every day and follow your provider’s advice.
6. Will hypothyroidism make it hard to lose weight even on treatment?
Weight may go down a little once thyroid levels are corrected, but many people still need attention to diet, sleep, and physical activity to manage weight. Thyroid medicine is not a weight‑loss drug; taking more than prescribed will not speed up weight loss and can be unsafe.
7. Can hypothyroidism affect cholesterol and heart health even if I feel fine?
Untreated or undertreated hypothyroidism can raise cholesterol levels and increase the risk of heart disease over time, sometimes without obvious symptoms. Getting thyroid levels into the target range often helps improve cholesterol and may reduce cardiovascular risk.
8. Is it safe to take supplements if I have hypothyroidism?
Some supplements, especially those containing iodine, biotin, iron, calcium, or “thyroid support” blends, can interfere with tests or with levothyroxine absorption. Always check labels and talk to your healthcare provider or pharmacist before starting new vitamins or herbal products.
9. Do I need to see an endocrinologist, or can my primary doctor manage this?
Many people with straightforward hypothyroidism are safely managed by a primary care provider with periodic blood tests and dose adjustments. Referral to an endocrinologist is often recommended in more complex situations, such as pregnancy, difficult‑to‑control levels, other endocrine diseases, or unusual test results.
10. How often should my thyroid levels be checked once I am stable?
After your dose is stable and symptoms are controlled, TSH is usually checked about once or twice a year, or sooner if you have new symptoms or major health changes. Testing is also repeated after changes in dose, new long‑term medications, significant weight change, or pregnancy.
Disclaimer: This information is for educational purposes only and does not replace medical advice, diagnosis, or treatment from your own healthcare provider.
Written by: Eden Grace Ramos-Arsenio, RN
Sources: National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK/NIH); Cleveland Clinic; NHS; Patient.info; American Thyroid Association (ATA); Healthdirect Australia; Mayo Clinic; peer‑reviewed medical and nursing journals.
